Our 15-year retrospective study of renal biopsies provides comprehensive data about demographics and the prevalence of kidney diseases in Hungary. Although our report was conducted in a single pathological center, it covers almost half of the Hungarian population and can therefore be generalized.
Our database has a slight female dominance, which might root in the fact that the male/female demographic ratio decreases with the increase of age15. However, the gender-based biopsy rate showed a relatively higher number of males who have gone under renal biopsy. This compares well with other European studies1.
The mean age was 44.2 ± 21.9 years, which coincides with similar reports in other registries so far1. The increase in biopsy samples from 2014 was partly due to the addition of other tertiary nephrology centers to the catchment area but the contribution of the increasingly aging population and subsequent higher biopsy rate in the elderly population cannot be disregarded either. This implies that there is a long-term outlook even for senior patients, and suggests an increasing life expectancy, giving an indirect hint of improving health care and social conditions16.
The average biopsy rate of 36.3 per one million person-years lags behind most of the European reports17, however, from 2015, our data collection rate has increased significantly and seems to be catching up. We assume many reasons behind the lower rates. First, the catchment area is scattered, and there are just a few hospitals that maintain a regular connection with the university pathological department. In addition, a conservative approach to biopsies may have caused the lower number of biopsy incidences. Financial considerations can also hold the biopsy rates back1,9. Nevertheless, biopsy rates in Hungary have significantly improved over the last few years. This may be due to several reasons. The decision to biopsy has been positively impacted by the increased proficiency and low complication rates of the procedure. This has resulted in increased ease of performing renal biopsy procedures by nephrologists and subsequently has led to improved biopsy skills. Additionally, nephrologists with higher expertise in performing renal biopsies, tend to have lower threshold for performing these procedures. Furthermore, nephrologists and associated professionals who feel more confident in their fellows’ competence are more likely to request more biopsies. The changing emphasis of performing a biopsy during medical training may also contribute to the increase in the biopsy rates. Training pattern has changed in the last decades, leading to a change in the nephrologist population. Many doctors who have trained abroad and those who have familiarized themselves with renal biopsy procedures during their training, become acquainted with it and are more likely to perform it. Thus, with time the biopsy rate could grow exponentially18. The widespread availability of the internet, medical search engines, and journals provide better availability of high-quality, up-to-date information on kidney diseases, and the utility of the biopsy, which also has contributed to the lowering threshold for renal biopsy. Nonetheless, we cannot exclude the real increase in the incidence of kidney diseases as a contributing factor to the increased renal biopsy rates as well as the aging population. With aging, certain kidney diseases and renal manifestations of systemic diseases may occur as they have more time to develop.
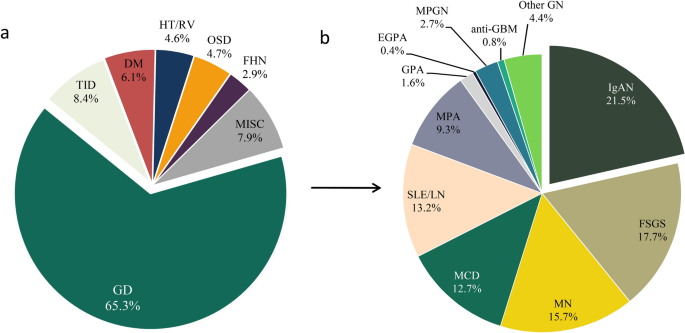
The results confirmed that glomerular diseases prevail over the other diagnoses similar to most of the registries3,8,17,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43. Within glomerular diseases, IgA nephropathy was the most common entity, which correlates well with another Hungarian registry in a different region44,45 and other registries in different countries2,3,4,5,6,8,9,19,20,21,29,30,31,46,47,48,49,50,51,52,53,54,55,56,57,58. Interestingly, there were some countries, mainly outside of Europe, where membranous nephropathy22,23,26,38,59,60 or FSGS/MCD were the most frequently diagnosed24,25,32,33,34,35,37,40,43,61,62,63,64,65,66,67,68,69,70. Membranoproliferative glomerulonephritis prevailed in Africa and mostly in Eastern countries7,27,28,39,43,71,72,73,74. In some countries, lupus nephritis, diffuse endocapillary glomerulonephritis, IgM nephropathy and familial/hereditary nephropathies dominated the renal biopsies36,41,75,76,77,78 (Fig. 5). The discrepancy of the most frequent diagnoses indicates not only a different genetic, lifestyle and environmental background but also raises awareness for the heterogeneity of the biopsy indications17.
Figure 5 Overview of the most frequent renal diseases in renal registries and studies around the world. Biopsy indication was heterogenous except in Cameroon, Senegal, Ghana, and Zaire, where only nephrotic syndrome was considered. Biopsies were performed on adults ± children, except Namibia, where only children were enrolled in the study. Information was not found from countries left white. This Figure was created with Paint software (Microsoft Windows 10 v20H2). The world map template was downloaded from https://www.dreamstime.com/royalty-free-stock-images-empty-world-map-image4506299 under Royalty-free license, Dreamstime LLC (Brentwood, TN, US). IgAN IgA nephropathy—histologically proven and Henoch-Schönlein purpura/nephritis, FSGS focal segmental glomerulosclerosis, MN membranous nephropathy (primary and secondary), MCD minimal change disease, SLE/LN systemic lupus erythematosus/lupus nephritis, MPGN membranoproliferative glomerulonephritis, Other GN other glomerulonephritis, FHN familial/hereditary nephropathies, MISC miscellaneous diseases. *Only children were examined. Full size image
Sine morbo diagnoses are mostly believed to be produced by the inherent problem of the sampling errors, resulting in false-negative samples, however, true negative cases cannot be ruled out either.
The key predictor of biopsy adequacy is the number of glomeruli, which changes depending on the kind of glomerular disease. In general, missing the impaired glomeruli in the sample is 10% if the bioptic sample includes 10 glomeruli and it drops to 1% if the sample contains 20 glomeruli. As a result, for an acceptable sample, at least 10 glomeruli are required79. This notion is supported by the recent guideline of the Kidney Disease: Improving Global Outcomes (KDIGO) organization on the management of glomerular diseases80. In case it is not yielded during the sampling, chances of missing the afflicted part of the kidney increase.
In our study, negative cases made up for 0.38% of the total biopsies. This rate varies between 0.3 and 8.5% in the international reports9,22,36,47,48,57,61,70. A biopsy is still the ‘gold standard’ for the diagnostic evaluation of glomerular diseases and the biopsy should be performed when the value of the information obtained from the biopsy exceeds the risk entailed80. Most of the renal biopsy indications (e.g. nephrotic syndrome, acute nephritic syndrome, affected kidney in systemic diseases, etc.) rule out the true negative results, hence these are characteristic for kidney diseases. This can explain the small rate of true negative samples compared to other diagnostic tests. Indications for renal biopsy in the countries where the report on negative samples was available, were generally similar. However, the number of the negative samples increased in direct proportion to the rate of biopsies. This correlation draws attention to the threshold for the execution of a renal biopsy: countries that perform a renal biopsy with more subtle clinical or laboratory abnormalities have a higher biopsy rate and increased number of negative histological results, while countries with low negative sample results and biopsy rate may interpret the indications rather strictly. In addition, local resources are also likely to determine the prevailing practice on performing kidney biopsies80.
The prevalence of hypertension increases with age81, and renal manifestation may be parallel this tendency. In this study, we found less hypertension/renovascular disease-related diagnosis in the biopsy trends despite the increasing age. This might indicate better medical support and blood pressure control for the patients, even in the elderly. On the other hand, we cannot exclude the dilution effect entirely: the rise of the biopsy rate may have contributed to a relatively lower number of hypertensive/renovascular main diagnosis. Here we must note that many specimens had arterial hyalinosis as a sign of hypertension which was not described as the main diagnosis if it was an indirect result or secondary effect. The hypertension/renal vascular main category represents the specimens if the signs of hypertension were explicit or no other pathognomic lesion was found.
The increase of age was accompanied by a surplus of microscopic polyangiitis, and a lower number of familial diseases. As indicated in other studies, the average age is over 50 years in MPA, indicating a higher prevalence in older patients82. The increasing number of LCDD and MPGN in the biopsy trends might be attributed to monoclonal gammopathies, which also rise with the aging population. MPGN, as a heterogeneous range of disorders, is often clinically under-recognized and hence, under-diagnosed83. Although monoclonal gammopathies may have a diverse and even distinct morphology, the most common pattern is MPGN84,85,86.
The number of membranous nephropathies showed increase with age and demonstrated a male dominance. This may be explained by the gradually aging population10 and the corresponding increase in the incidence of malignancies87. This finding correlates well with international studies88. Nevertheless, the increasing level of air pollutants cannot be excluded either89. We demonstrated a slightly higher proportion of MN cases than in the neighboring countries, which may be attributed to our worldwide number one ranking in lung and colorectal cancers and a superior place in ovarian and bladder cancers90. We also proved that MN occurs at a younger age in males which may be attributed to their lower participation in screening tests, worse diet, and lifestyle differences91. It is also worth noting that the availability of anti-PLA2R (phospholipase-A-2-receptor) titer measurements widened our diagnostic arsenal, and in some situations may lead to a decrease in the biopsy incidence in primary MN cases92.
Younger patients were burdened more by lupus nephritis, IgA nephropathy, minimal change disease, and focal segmental glomerulosclerosis. The relative early manifestation of these diseases suggests the possibility of genetic involvement.
The prevalence of diabetic nephropathy varied in the reviewed articles. Its overall prevalence in this study was higher than in most countries17. It is worth noting that the population in Hungary has one of the highest overweight and obesity rates in Europe15. On the other hand, a Western German study3 showed a 3.6-fold higher rate of diabetic nephropathy in their study. The discrepancies suggest a variance in the indications of biopsy. The relatively low incidence of diabetic nephropathy in our study compared to theirs may be due to the fact that performing a renal biopsy in diabetes mellitus is necessary only when an unexpectedly high rate of proteinuria or renal function decline is present. However, early stages of diabetic nephropathy may present with advanced structural damage despite the fairly normal kidney function93. This suggests that approaching biopsy indications with a less restrictive attitude may be advantageous and draws attention to the poor secondary prevention measures in Hungary.
MPA is known to have a rather even gender distribution94. According to some reports, it has a slight male predominance95,96,97. However, gross comparison in our study showed a significant female dominance. This cannot be explained only by the shrinking number of males with age, since we observed female dominance in all age groups. It raises attention to the possibility, that although MPA is equal and even a bit more frequent in males, the renal manifestation may be affected by gender, and may occur more often in females.
The female dominance of amyloidosis is associated with the female dominance of AA amyloidosis. Most of the patients with this diagnosis had an underlying rheumatoid arthritis, which is more frequent in females. The rest was associated with inflammatory bowel diseases. AA amyloidosis also reflects the prevalence of chronic inflammatory conditions over time.
Furthermore, in this study, the incidence of ANCA-associated glomerulonephritis increased over time. This trend correlates well with previous reports in other epidemiologic studies98,99,100. ANCA-associated vasculitis is more prevalent in the older population101, therefore the aging population could explain its increasing incidence. The increased incidence may also be attributed to an actual increase in incidence, change in classification criteria, and wider availability of diagnostic ANCA serology tests102,103. Moreover, increased recognition may be due to increased awareness by the clinicians because of a more thorough education98.
Due to the COVID-19 pandemic, the healthcare system had a major challenge worldwide. Accordingly, in 2020 the renal biopsy rate was lower, compared to the previous years. Many Hungarian nephrology departments had to switch to urgent care for patients with COVID-19 from March to May and November to December in 2020, which reduced the number of biopsies that otherwise could have been performed. In addition, patients with less severe symptoms and stable kidney disease avoided hospital visits due to fear of the coronavirus. We hypothesized that during the pandemic only the portion of kidney diseases with rapid progression or severe symptoms, and for which treatment needed a histopathological confirmation ended up in biopsies. Of course, serology results with these patients were non-contributory. This underlines the diagnostic value and indication for biopsies even in these difficult times. Although our database did not have large case numbers in 2020, we found that the rate of MN decreased significantly. In the primary forms of MN where the anti-PLA2R is present, renal biopsies could be disregarded, especially in a pandemic situation. The rise of GPA can be explained partly by the better awareness of the disease, but the effect of the pandemic cannot be excluded either. More data are needed in the future to explain this trend of the disease.
Many countries run renal biopsy registries to have a more comprehensive insight into epidemiologic data, to improve research possibilities5,9,20,24,47,49,50,51,55,61,104. These registries also contain clinical data which can enhance a more in-depth understanding of the diseases. Recently the Hungarian Society of Nephrology has also established a renal biopsy registry, which will aid to conduct clinicopathological research. To this end with this article, we would also like to take the initiative to develop a high-functioning database and encourage both clinicians and pathologists to take a share of filling an international biopsy registry, which would be very important quality feedback to our overall clinical work.
Our retrospective study presents the long-term trends in kidney diseases diagnosed by renal biopsy in Hungary. The diagnostic trends in our database showed increasing biopsy rates among the elderly and the growing frequencies of age-related diseases. Trends of 2020 showed that the availability of kidney biopsies reduced during the COVID-19 pandemic, but renal biopsy remained an important diagnostic tool even in difficult times.
The establishment of not only national but international kidney biopsy registries should be encouraged and supported by scientific societies, as it is very important to compare these trends internationally, which can help to improve the quality control of nephrology care worldwide.
https://www.nature.com/articles/s41598-021-04274-9